
What is the main idea of drive theory? Drive theory posits that behavior is primarily motivated by biological needs and the inherent drive to maintain homeostasis. This foundational theory, developed over decades with contributions from figures like Clark Hull and Sigmund Freud, explains how internal states of tension (drives) propel organisms towards actions that reduce these tensions and restore equilibrium.
Understanding drive theory requires exploring concepts like homeostasis, drive reduction, and the categorization of drives into primary (biological) and secondary (learned) types. This exploration will delve into the theory’s strengths, weaknesses, and its continuing relevance in explaining human motivation in the 21st century.
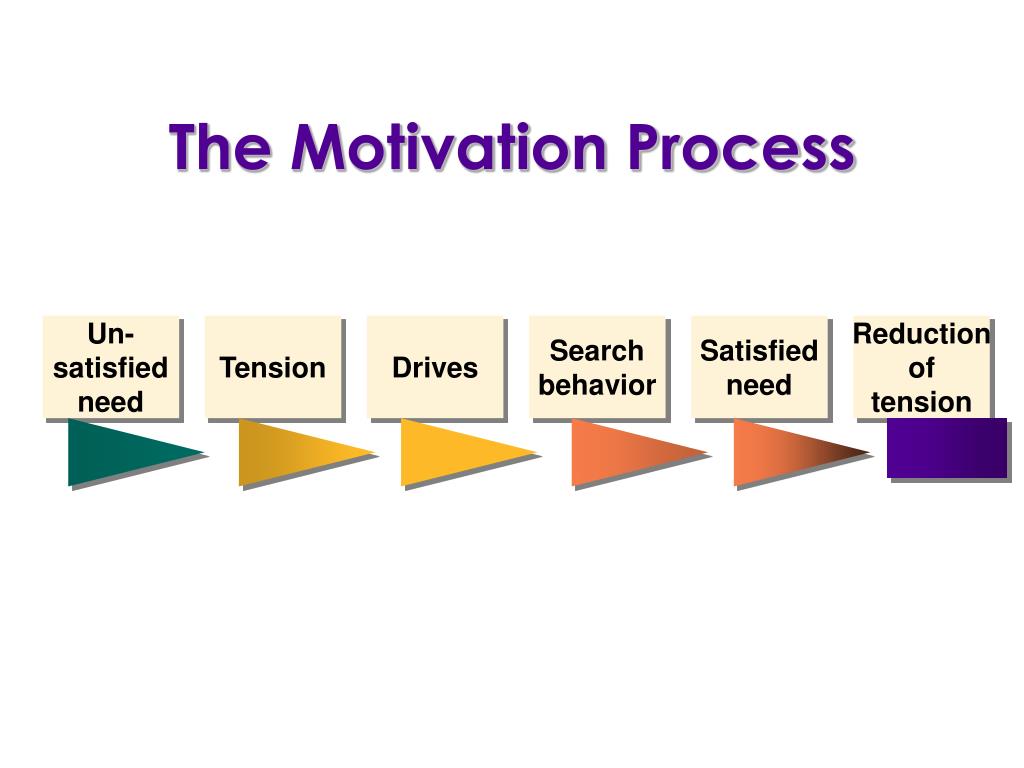
The core principle is the organism’s inherent push towards equilibrium. A disruption in this equilibrium, caused by unmet biological needs (like hunger or thirst), creates a drive state. This drive state motivates behavior aimed at reducing the tension and restoring homeostasis. For example, hunger (a drive) motivates eating (behavior) to reduce the drive and restore blood glucose levels. The theory also distinguishes between primary drives, rooted in biological needs, and secondary drives, learned through association and conditioning.
The interplay between these drives, their biological underpinnings, and the influence of individual differences forms the basis of a comprehensive understanding of drive theory.
Drive Theory Fundamentals: What Is The Main Idea Of Drive Theory
Drive theory, a cornerstone of motivational psychology, posits that internal biological needs drive behavior. This theory offers a compelling framework for understanding how our bodies’ inherent requirements influence our actions, shaping our daily lives in profound ways.
Core Principles of Drive Theory
Drive theory rests on three fundamental concepts: homeostasis, drive reduction, and the role of biological needs. Homeostasis refers to the body’s tendency to maintain a stable internal environment. Drive reduction describes the process of alleviating these imbalances, and biological needs are the underlying physiological requirements that initiate this process.
- Homeostasis: The body’s natural equilibrium. Examples include maintaining a stable body temperature (thermoregulation), regulating blood glucose levels, and balancing fluid levels. If any of these systems become imbalanced, the body initiates actions to restore equilibrium. For instance, shivering when cold, sweating when hot, and feeling thirsty when dehydrated all represent homeostatic mechanisms in action.
- Drive Reduction: The process of reducing physiological arousal or tension. Examples include eating to reduce hunger, drinking to reduce thirst, and sleeping to reduce fatigue. These actions directly address the underlying biological need, reducing the associated drive state.
- Biological Needs and Motivation: These are the fundamental physiological requirements that trigger drives. Examples include the need for food, water, and sleep. The strength of the drive is often proportional to the intensity of the biological need; the more dehydrated you are, the stronger the drive to drink becomes.
Biological Basis of Drives
Drive theory posits that internal states of tension or arousal motivate behavior. Understanding the biological underpinnings of these drives—hunger, thirst, and sexual motivation—is crucial to comprehending their influence on our actions and overall well-being. These drives are not simply psychological constructs; they are deeply rooted in complex physiological processes involving hormonal and neurotransmitter systems, specific brain regions, and intricate feedback loops.
Physiological Mechanisms Underlying Drives
The intricate interplay of hormones and neurotransmitters orchestrates the experience and regulation of hunger, thirst, and sexual drive. These chemical messengers act on specific brain regions to initiate and modulate these fundamental drives.
- Hunger: Ghrelin, a hormone produced in the stomach, stimulates appetite. Leptin, released by fat cells, signals satiety. Insulin, secreted by the pancreas, facilitates glucose uptake into cells, influencing blood sugar levels and hunger. The hypothalamus, particularly the lateral and ventromedial nuclei, plays a crucial role in integrating these signals and regulating food intake. Dopamine and serotonin, neurotransmitters associated with reward and mood, respectively, also influence food seeking and consumption.
- Thirst: Vasopressin, released by the pituitary gland, conserves water by reducing urine output. Angiotensin II, a hormone produced in response to low blood volume, stimulates thirst. The hypothalamus, particularly the organum vasculosum of the lamina terminalis (OVLT), detects changes in blood osmolarity (solute concentration) and blood volume, triggering thirst. Dopamine and serotonin also modulate the experience and behavior associated with thirst.
- Sexual Drive: Testosterone in males and estrogen in females are crucial hormones for sexual motivation and function. The hypothalamus, amygdala, and prefrontal cortex (PFC) are key brain regions involved in sexual behavior, processing emotional and cognitive aspects of sexual drive. Dopamine is a significant neurotransmitter in the reward pathway associated with sexual activity, while serotonin influences sexual behavior and satiety.
Homeostasis and Drive Regulation
Homeostasis, the body’s tendency to maintain internal equilibrium, is central to drive regulation. Each drive operates within a homeostatic set point, a target range for a physiological variable (e.g., blood glucose, blood volume, hormonal levels). Deviations from this set point trigger feedback mechanisms to restore balance.
Brother, the core of drive theory, as I understand it, rests on the idea that internal states of tension motivate behavior; we seek to reduce this tension. Think of it like this: our spiritual quests, our yearning for knowledge, are also drives. To effectively manage this pursuit of knowledge, consider building a self hosted knowledge base ; it’s a tool to organize and reduce the tension of unanswered questions, thus aligning perfectly with the central tenet of drive theory – the reduction of internal conflict through action.
- Hunger: Low blood glucose levels trigger the release of ghrelin, stimulating appetite and food intake. As blood glucose rises after eating, leptin is released, signaling satiety and reducing appetite.
- Thirst: Dehydration, reflected in increased blood osmolarity and decreased blood volume, triggers the release of vasopressin and angiotensin II, stimulating thirst and water intake. As blood volume and osmolarity return to normal, thirst diminishes.
- Sexual Drive: Hormonal fluctuations influence sexual drive, with higher levels of testosterone or estrogen typically associated with increased libido. Feedback mechanisms involving neurotransmitters like dopamine and serotonin regulate the experience of sexual arousal and satiety.
Genetic Influence on Drive Strength and Regulation
Genetic factors significantly contribute to individual differences in drive strength and regulation. Variations in genes influencing hormone production, receptor sensitivity, and neurotransmitter pathways can affect appetite, thirst, and libido. While specific genes are still under investigation, research points to the influence of genetic polymorphisms on appetite regulation and predisposition to eating disorders, for instance. Similar research is ongoing regarding the genetic basis of variations in thirst response and sexual drive.
Role of the Nervous System in Drive Regulation
The nervous system plays a pivotal role in sensing internal bodily states, processing this information, and initiating appropriate behavioral responses.
- Hypothalamus: Acts as a central integrating center, receiving input from various peripheral sensors and regulating the release of hormones that influence drive states.
- Amygdala: Processes emotional aspects of drives, particularly the motivational and reward components.
- Hippocampus: Involved in the memory aspects of drives, influencing learned associations between stimuli and drive-related behaviors.
Neural pathways relay information about internal states (e.g., low blood glucose, dehydration) to the brain, triggering the conscious experience of hunger, thirst, or sexual arousal. These pathways also mediate the motor responses involved in satisfying these drives (e.g., seeking food, drinking water, engaging in sexual behavior). The autonomic nervous system, specifically the sympathetic and parasympathetic branches, mediates the physiological responses accompanying these drives (e.g., increased heart rate and blood pressure during arousal, relaxation after satiety).
Diagram Illustrating the Interaction Between Biological Needs and Drive States
[Imagine a flowchart here. It would begin with a box labeled “Biological Need” (e.g., low blood glucose). An arrow would lead to a box labeled “Sensory Input” (e.g., glucose receptors in the liver). Another arrow would lead to a box labeled “Hypothalamus” (integrating center). Arrows would then branch out to boxes labeled “Hormonal Response” (e.g., ghrelin release), “Neurotransmitter Response” (e.g., dopamine release), and “Drive State” (e.g., hunger).
Finally, an arrow would lead to a box labeled “Behavioral Response” (e.g., eating). Feedback loops would be shown with arrows looping back from the “Behavioral Response” to the “Biological Need,” representing the restoration of homeostasis. Different colors could be used to represent sensory input (blue), central processing (red), and motor output (green). The flowchart would be repeated for thirst and sexual drive, highlighting the different hormones, neurotransmitters, and brain regions involved.]The diagram illustrates the cyclical nature of drive regulation.
Biological needs trigger sensory input that is processed by the brain, leading to hormonal and neurotransmitter responses, the conscious experience of a drive state, and ultimately, behavioral responses that address the initial need. Feedback loops ensure that the system returns to homeostasis once the need is met.
Comparative Analysis of Hunger, Thirst, and Sexual Drive
The table below summarizes the similarities and differences in the physiological mechanisms underlying hunger, thirst, and sexual drive. While all three involve hormonal and neurotransmitter systems and specific brain regions, the specific components and their interactions vary significantly.
| Feature | Hunger | Thirst | Sexual Drive |
|---|---|---|---|
| Key Hormones | Ghrelin, Leptin, Insulin | Vasopressin, Angiotensin II | Testosterone, Estrogen |
| Key Neurotransmitters | Dopamine, Serotonin | Dopamine, Serotonin | Dopamine, Serotonin |
| Key Brain Regions | Hypothalamus, Amygdala | Hypothalamus, Amygdala | Hypothalamus, Amygdala, Prefrontal Cortex |
| Homeostatic Set Point | Blood Glucose Level | Blood Osmolality, Blood Volume | Hormonal Levels, Neurotransmitter Balance |
Clinical Implications of Drive Dysregulation
Disruptions in the homeostatic mechanisms regulating drives can lead to various disorders.
- Anorexia Nervosa and Bulimia Nervosa: These eating disorders involve severe disturbances in eating behavior and body image, often associated with dysregulation of appetite hormones and neurotransmitters, impacting the hypothalamus and other brain regions.
- Diabetes Insipidus: Characterized by excessive thirst and urination, it results from a deficiency in vasopressin production or action, disrupting the body’s ability to conserve water.
- Hypogonadism: Defined by deficient sex hormone production, it can lead to reduced libido and impaired sexual function, reflecting dysregulation in the hypothalamic-pituitary-gonadal axis.
These disorders highlight the profound impact of drive dysregulation on physical and psychological well-being. The consequences range from nutritional deficiencies and dehydration to significant emotional distress and impaired social functioning. Understanding the underlying biological mechanisms is crucial for developing effective treatments and interventions.
Drive Reduction and Homeostasis
Drive reduction theory posits that a biological need creates an unpleasant state of tension, or drive, motivating an organism to engage in behaviors that reduce this tension and restore equilibrium. This equilibrium, or stable internal state, is known as homeostasis. The theory emphasizes the crucial role of negative feedback mechanisms in regulating physiological processes and maintaining balance.Drive reduction and homeostasis are intrinsically linked.
A drive represents a deviation from homeostasis, a disruption of the body’s internal balance. This deviation triggers a physiological response aimed at reducing the drive and restoring homeostasis. The strength of the drive is directly proportional to the degree of deviation from the optimal internal state. This process is cyclical: need -> drive -> drive-reducing behavior -> homeostasis.
Examples of Homeostasis through Drive Reduction
The body employs numerous mechanisms to maintain homeostasis through drive reduction. For instance, thirst acts as a drive triggered by dehydration, a deviation from the optimal fluid balance. This drive motivates behaviors such as drinking water, which reduces the drive and restores homeostasis by replenishing fluid levels. Similarly, hunger, driven by low blood glucose levels, motivates food intake, thereby restoring energy balance and alleviating the hunger drive.
Drive theory, in its essence, posits that our actions stem from internal states seeking equilibrium. Think of it like a compass always pointing North; our behavior is similarly driven by biological needs. Consider how this relates to the broader understanding of the universe; even the seemingly disparate question of whether 5th graders learn about both geocentric and heliocentric models, as explored in this resource do 5th graders learn about geo and heliocentric theory , reflects a similar pursuit of understanding our place within a larger system.
Ultimately, drive theory suggests that our quest for knowledge, like our biological needs, motivates our actions.
Another example is thermoregulation; when body temperature falls below the optimal range, shivering generates heat, reducing the drive for warmth and restoring thermal homeostasis. Conversely, sweating helps cool the body when it’s too hot. These examples highlight the body’s intricate mechanisms for maintaining internal stability.
Comparison of Drive Reduction Models, What is the main idea of drive theory
Several models exist within the framework of drive reduction theory, offering slightly different perspectives. While all emphasize the role of drives in motivating behavior to restore homeostasis, they vary in their emphasis on specific factors. Some models focus primarily on biological needs and physiological feedback mechanisms, emphasizing the purely biological aspects of drive reduction. Other models incorporate learning and cognitive factors, acknowledging that learned associations and expectations can influence drive-reducing behaviors.
For instance, a learned aversion to a particular food might override the biological drive for hunger, demonstrating the interaction between biological and cognitive influences. Still other models emphasize the importance of incentives and rewards in shaping behavior, suggesting that the anticipation of pleasure or reward can further motivate drive-reducing actions. The differences between these models highlight the complexity of the drive reduction process and the multifaceted nature of motivation.
Drive and Motivation

Drive theory posits that internal states of tension, or drives, motivate behavior aimed at reducing that tension and achieving homeostasis. However, motivation is a broader concept encompassing a wider range of influences beyond purely physiological drives. Understanding the nuances of this relationship is crucial to a comprehensive understanding of behavior.Drives are a specific subset of motivational factors, primarily stemming from biological needs.
Other motivational factors, such as incentives, goals, and emotions, are less directly tied to physiological needs and can be significantly influenced by cognitive and social factors. For instance, the drive to eat is directly linked to hunger pangs and energy depletion, whereas the motivation to achieve a promotion is influenced by factors like ambition, social status, and financial security.
While drives are powerful motivators, their influence is often interwoven with other motivational forces.
Differences Between Drives and Other Motivational Factors
Drives are characterized by their biological basis and their inherent push towards homeostasis. They are often involuntary and relatively inflexible. In contrast, other motivational factors, such as intrinsic motivation (driven by internal rewards) or extrinsic motivation (driven by external rewards), can be more consciously controlled and flexible. The pursuit of a hobby, for example, might be intrinsically motivated, while the pursuit of a financial bonus is extrinsically motivated.
These non-drive motivations can override or interact with drives in complex ways. For example, a person might skip a meal (neglecting the drive for food) due to a strong intrinsic motivation to finish a project.
Influence of Drives on Behavior
Drives exert a powerful influence on behavior by creating an internal state of tension or arousal. This arousal motivates individuals to engage in behaviors that are likely to reduce this tension. The intensity of the drive, as well as the perceived likelihood of success in reducing the drive, will influence the strength of the motivated behavior. For instance, a strong thirst drive (high arousal) will lead to more vigorous searching for water than a mild thirst drive (low arousal).
Furthermore, if an individual believes finding water is unlikely (low perceived likelihood of success), the motivated behavior might be less intense than if finding water is perceived as likely. This interplay between drive intensity and perceived likelihood of success significantly shapes the behavioral response.
Intrinsic and Extrinsic Motivation Related to Drives
The following table illustrates the distinction between intrinsic and extrinsic motivation in the context of drive theory:
| Type of Motivation | Example related to Drive Theory |
|---|---|
| Intrinsic Motivation | A runner experiences a “runner’s high” (endorphin release), intrinsically rewarding the act of running and reinforcing the behavior even beyond the drive to maintain physical fitness. |
| Extrinsic Motivation | A person drinks water not only because of the thirst drive (biological need), but also to receive a reward (e.g., a prize for completing a hydration challenge), which provides an extrinsic motivation to drink. |
Drive Theory and Learning
Drive theory posits that internal states of tension, or drives, motivate organisms to engage in behaviors that reduce those tensions and restore equilibrium. This inherent link between internal states and behavior has significant implications for understanding how we learn. Learning, in essence, is the process of acquiring new knowledge or behaviors, and drive theory provides a framework for understanding how motivational factors influence this process.Drive theory suggests that the strength of a drive directly impacts the intensity and persistence of learning-related behaviors.
A strong drive, like intense thirst or hunger, creates a heightened state of arousal that focuses attention and energizes actions aimed at satisfying that drive. Conversely, a weak drive may result in less focused and less persistent learning efforts. This relationship is not simply about motivation; it’s about the very mechanisms by which we learn and retain information.
The Influence of Drives on Learning Behaviors
Drives significantly influence the types of learning behaviors an organism exhibits. For example, a hungry rat will learn more quickly to navigate a maze if the reward at the end is food compared to a situation where the reward is less relevant to its drive state. Similarly, a thirsty animal will learn faster to obtain water than to obtain a less immediately needed reward.
These examples illustrate how drives prioritize certain learning behaviors over others, reflecting the organism’s immediate needs. The strength of the drive acts as a filter, emphasizing information and actions directly related to drive reduction.
Reinforcement and Punishment in Drive-Related Learning
The principles of reinforcement and punishment are central to understanding how drives shape learning through experience. Positive reinforcement, such as receiving food after completing a task, strengthens the association between the behavior and the drive reduction. This leads to an increase in the likelihood of repeating the behavior in the future. Negative reinforcement, on the other hand, involves the removal of an aversive stimulus (e.g., escaping a painful situation) after performing a specific behavior.
This too increases the likelihood of the behavior being repeated as it is associated with the removal of an unpleasant state. Punishment, conversely, weakens the association between a behavior and drive reduction. For example, if a rat receives an electric shock after attempting a specific action, it’s less likely to repeat that action in the future, even if it was initially associated with drive reduction.
The effectiveness of reinforcement and punishment depends on the strength of the drive and the timing and consistency of the reinforcement or punishment. A consistently delivered reward will be more effective in shaping behavior than an intermittent or unpredictable one.
Drive Theory and Emotion
Drive theory, while primarily focusing on biological needs and their motivational consequences, is inextricably linked to emotional experience. The satisfaction or frustration of drives elicits a range of emotional responses, shaping our behavior and physiological state. Understanding this interplay is crucial for a complete understanding of motivation and human behavior.
The Connection Between Drives and Emotional Responses
Biological drives and their associated emotional responses are deeply intertwined. The experience of hunger, for instance, isn’t simply a physiological sensation; it’s accompanied by emotions ranging from mild discomfort to intense cravings and even anger if access to food is blocked. Similarly, thirst evokes anxiety and irritability when unmet, while sexual drive is linked to a spectrum of emotions from pleasure and intimacy to frustration and rejection.
These emotional experiences are not merely epiphenomena but integral components of the drive process, influencing its intensity and how we respond to it. Neurologically, the limbic system, particularly the amygdala and hypothalamus, plays a key role in processing both emotional and drive-related information. The amygdala, involved in processing fear and other emotions, can influence the intensity of hunger or thirst drives in stressful situations.
The hypothalamus, a crucial center for regulating homeostasis, also plays a central role in the neurobiological underpinnings of drives and emotions. For example, the release of hormones like cortisol during stress can suppress appetite, illustrating the interplay between the emotional and drive systems.
| Drive | Positive Emotions | Negative Emotions | Physiological Responses |
|---|---|---|---|
| Hunger | Satisfaction, Pleasure, Contentment | Frustration, Anger, Anxiety, Irritability | Increased ghrelin, decreased leptin, stomach contractions, increased blood glucose |
| Thirst | Relief, Satisfaction | Anxiety, Frustration, Irritability, Dehydration symptoms | Dry mouth, increased thirst sensation, decreased blood volume, increased vasopressin |
| Sexual Drive | Pleasure, Intimacy, Love, Excitement | Frustration, Anxiety, Rejection, Shame, Guilt | Increased libido, physiological arousal, release of endorphins and oxytocin |
Emotional States’ Influence on Drive-Related Behaviors
The initiation, intensity, and cessation of drive-related behaviors are significantly influenced by emotional states. Both positive and negative emotions can modify our responses to biological needs.
- Fear, for example, can suppress appetite (leading to decreased food intake) and increase cravings for comfort foods (leading to increased intake of specific foods).
- Conversely, happiness can enhance sexual desire and increase the likelihood of engaging in sexual activity.
- Cognitive appraisal plays a vital role in mediating the impact of emotions on drives. For instance, the perception of a situation as threatening (cognitive appraisal) can trigger a fear response that suppresses hunger, even if the physiological need for food remains.
Emotional regulation strategies, such as mindfulness or relaxation techniques, can directly affect drive behaviors. By managing stress and anxiety, individuals can mitigate the negative impact of these emotions on appetite and other drives. Conversely, cultivating positive emotions can enhance motivation and engagement in activities related to satisfying drives.
Physiological Changes Associated with Drives and Emotions
Drives and emotions share overlapping physiological responses, but key differences exist. Both involve the autonomic nervous system, but the patterns of activation differ significantly.
Key Differences in Physiological Responses: While both drives and emotions involve complex physiological changes, the specific patterns differ significantly. Drives often involve more localized changes related to the specific bodily need (e.g., stomach contractions for hunger), whereas emotions often involve more widespread changes across the body, including cardiovascular, respiratory, and endocrine systems. For instance, hunger primarily involves the gastrointestinal system, while fear activates the sympathetic nervous system, leading to increased heart rate, respiration, and release of adrenaline.
Hormonal changes also differ. Hunger is associated with fluctuations in ghrelin and leptin, while fear and anxiety involve increased cortisol levels. Neurotransmitter activity also varies, with dopamine playing a key role in reward and pleasure associated with drive satisfaction, while norepinephrine and serotonin are involved in the regulation of emotional responses.
A Hypothetical Scenario Illustrating Drive-Emotion Interaction
Imagine a person (Sarah) who is intensely thirsty (drive) after a strenuous hike. However, she also feels anxious (emotion) because she’s lost and unsure of her location. Her anxiety might suppress her immediate drive to drink. Her heart races (sympathetic nervous system activation due to anxiety), making it difficult to focus on the immediate need for water. She might delay seeking water, prioritizing dealing with her fear and finding a safe place before addressing her thirst.
This illustrates how a strong emotion can temporarily override a basic drive. Even when she finds water, her anxiety might affect how much she drinks or how quickly she consumes it.
Individual Differences in Drives
Drive theory, while providing a foundational understanding of motivation, doesn’t account for the significant variability observed in drive strength and expression across individuals. This section delves into the multifaceted factors contributing to these individual differences, encompassing genetic predispositions, neurological and hormonal influences, and the impact of personality and cultural context.
Factors Contributing to Individual Variations in Drive Strength
Individual variations in drive strength are a complex interplay of inherited traits, neurological mechanisms, and hormonal influences. Understanding these factors is crucial for a more nuanced perspective on motivation.
Genetic Predisposition
Genetic factors significantly influence the strength of various drives. Specific genes contribute to individual differences in reward sensitivity, influencing the intensity of drives like hunger, thirst, and achievement. For example, variations in the dopamine receptor gene (DRD2) have been associated with differences in reward sensitivity and thus, the strength of reward-driven behaviors. Similarly, genes related to appetite regulation, such as those influencing leptin and ghrelin levels, directly impact hunger drive strength.
The following table summarizes known genetic associations with drive strength:
| Drive Type | Gene(s) Involved | Effect on Drive Strength | Reference |
|---|---|---|---|
| Hunger | Leptin receptor gene (LEPR), Ghrelin gene (GHRL) | Variations affect appetite regulation, influencing hunger drive | [Citation needed: A relevant peer-reviewed study on leptin and ghrelin genes and hunger] |
| Thirst | [Gene(s) related to fluid balance regulation needed] | [Effect on thirst drive strength needed] | [Citation needed: A relevant peer-reviewed study on genes and thirst] |
| Achievement | Dopamine receptor gene (DRD2), Serotonin transporter gene (SLC6A4) | Variations affect reward sensitivity and emotional regulation, impacting achievement motivation | [Citation needed: A relevant peer-reviewed study on dopamine and serotonin genes and achievement motivation] |
Neurological Factors
Neurotransmitter systems and specific brain regions play a critical role in regulating drive strength. Dopamine, for instance, is central to the reward pathway, influencing the experience of pleasure and motivation. The hypothalamus, a key brain region involved in homeostasis, regulates drives like hunger and thirst. The amygdala processes emotions, impacting the intensity of emotionally driven behaviors. A simplified flowchart illustrating the reward pathway follows:[Flowchart description: The flowchart would begin with a stimulus (e.g., food, social interaction, achievement).
This would lead to activation of the ventral tegmental area (VTA), which releases dopamine. Dopamine would then travel along the mesolimbic pathway to the nucleus accumbens, amygdala, and hippocampus, resulting in feelings of pleasure, reward, and motivation. The prefrontal cortex would then evaluate the reward and influence subsequent behavior.]
Hormonal Influences
Hormones exert significant influence on drive strength. Testosterone, often associated with aggression and dominance, can increase the strength of power-seeking drives. Cortisol, a stress hormone, can suppress certain drives, particularly those requiring sustained effort or risk-taking. The following table compares the effects of different hormones on various drives:
| Hormone | Drive Type | Effect | Reference |
|---|---|---|---|
| Testosterone | Aggression, Competition | Increases drive strength | [Citation needed: A relevant peer-reviewed study on testosterone and aggression] |
| Cortisol | Achievement, Exploration | Decreases drive strength under chronic stress | [Citation needed: A relevant peer-reviewed study on cortisol and achievement motivation] |
| Estrogen | Affiliation | May influence affiliative behaviors | [Citation needed: A relevant peer-reviewed study on estrogen and affiliation] |
Drive Theory and Psychological Disorders
Drive theory, while offering a foundational understanding of motivation, also illuminates the pathways to psychological distress when the mechanisms regulating drives malfunction. Disruptions in the delicate balance of drive regulation, particularly concerning hunger, reward, and attachment, can significantly contribute to the development and maintenance of various psychological disorders. Understanding these disruptions is crucial for developing effective therapeutic interventions.
Disruptions in Drive Regulation and Psychological Disorders
The intricate interplay between biological drives and psychological well-being is evident in several mental health conditions. Homeostatic imbalances, particularly concerning the drive for hunger and satiety, are central to eating disorders. Similarly, dysregulation of reward pathways underlies addiction, while disturbances in the drive for affiliation and attachment contribute significantly to personality disorders. These dysregulations are often underpinned by complex neurobiological mechanisms, involving neurotransmitter imbalances and structural changes in the brain.
Homeostatic Imbalance in Eating Disorders
Eating disorders like anorexia nervosa and bulimia nervosa represent profound disruptions in the homeostatic regulation of hunger and satiety. Anorexia nervosa involves a severe restriction of food intake, driven by a distorted body image and an intense fear of weight gain. This behavior disrupts the body’s natural feedback loops, leading to hormonal imbalances, such as decreased leptin (a hormone signaling satiety) and increased ghrelin (a hormone stimulating hunger), further exacerbating the condition.
Neurobiologically, serotonin dysregulation plays a crucial role, influencing mood, appetite, and impulse control. Bulimia nervosa, characterized by cycles of binge eating followed by compensatory behaviors (purging), also involves disruptions in these neurochemical pathways, with additional involvement of dopamine and norepinephrine systems related to reward and stress response. The interplay of these neurobiological factors, coupled with psychological and environmental influences, creates a complex picture of eating disorder etiology.
Disrupted Reward Pathways and Addiction
Addiction, encompassing substance use disorders and behavioral addictions like gambling, stems from a fundamental dysregulation of the brain’s reward system. The dopamine system, central to experiencing pleasure and reinforcement, plays a critical role. Addictive substances or behaviors hijack this system, leading to intense cravings and compulsive seeking behaviors. The brain adapts to the excessive dopamine stimulation, resulting in tolerance (requiring increasing amounts of the substance or behavior for the same effect) and withdrawal symptoms upon cessation.
Different addictions may involve distinct neurotransmitter systems; for example, opioid addiction significantly impacts opioid receptors, while alcohol addiction affects GABAergic systems. The common thread, however, remains the dysregulation of reward pathways and the resulting compulsive pursuit of the addictive substance or behavior, irrespective of negative consequences.
Drive for Affiliation and Attachment in Personality Disorders
Disruptions in the drive for affiliation and attachment significantly impact the development of personality disorders. These disorders are characterized by enduring patterns of inner experience and behavior that deviate markedly from cultural expectations, causing distress or impairment. For example, individuals with avoidant personality disorder struggle with intimacy and fear rejection, reflecting a dysregulation in their drive for affiliation and secure attachment.
Those with borderline personality disorder exhibit unstable relationships and intense fear of abandonment, stemming from insecure and often traumatic attachment experiences. These patterns reflect maladaptive coping mechanisms developed in response to early relational experiences that disrupted the development of secure attachment, impacting emotional regulation and interpersonal functioning. The neurobiological underpinnings often involve dysfunction in areas of the brain associated with emotional processing and social cognition.
Examples of Psychological Disorders Linked to Drive Dysregulation
The table below provides specific examples of psychological disorders linked to dysregulation of various drives. The specific manifestations of dysregulation and the neurobiological correlates vary across disorders, highlighting the complexity of these conditions.
| Psychological Disorder | Affected Drive(s) | Specific Manifestations of Dysregulation | Neurobiological Correlates |
|---|---|---|---|
| Anorexia Nervosa | Hunger, thirst, self-preservation | Restriction of food intake, distorted body image, fear of weight gain | Dysregulation of leptin, ghrelin, serotonin |
| Bulimia Nervosa | Hunger, satiety, self-esteem | Binge eating followed by compensatory behaviors (purging), feelings of guilt and shame | Dysregulation of serotonin, dopamine, norepinephrine |
| Substance Use Disorder | Reward, pleasure, escape | Craving, compulsive drug seeking, tolerance, withdrawal | Dysregulation of dopamine, opioid, GABA systems |
| Obsessive-Compulsive Disorder (OCD) | Anxiety reduction, control | Repetitive thoughts (obsessions) and behaviors (compulsions) aimed at reducing anxiety | Dysregulation of serotonin, glutamate |
| Pathological Gambling | Reward, excitement, escape | Compulsive gambling despite negative consequences, financial ruin, relationship problems | Dysregulation of dopamine, reward pathways |
Therapeutic Interventions for Drive-Related Problems
Effective treatment for drive-related psychological disorders necessitates a multi-faceted approach targeting both the biological and psychological aspects of drive dysregulation. Therapeutic interventions aim to restore homeostatic balance, modify maladaptive behaviors, and enhance coping mechanisms.Therapeutic approaches for eating disorders often combine various techniques. Cognitive behavioral therapy (CBT) helps identify and modify maladaptive thoughts and behaviors related to food and body image, addressing cognitive distortions and promoting healthier eating patterns.
Dialectical behavior therapy (DBT) focuses on emotional regulation and distress tolerance, particularly helpful in managing intense emotions associated with eating disorders. Family-based therapy (FBT) involves the family in the treatment process, improving communication and support, essential for long-term recovery.Substance use disorders benefit from medication-assisted treatment (MAT), which reduces withdrawal symptoms and cravings, combined with behavioral therapies. Motivational interviewing helps individuals identify their reasons for change and develop strategies for overcoming barriers to recovery.
Relapse prevention strategies equip individuals with skills to manage cravings and high-risk situations, crucial for maintaining long-term abstinence.For personality disorders, psychodynamic therapy explores unconscious patterns and early relational experiences that contribute to maladaptive drive patterns, fostering insight and promoting healthier interpersonal relationships. Attachment-based therapies focus on repairing insecure attachments and developing secure relational patterns, improving emotional regulation and enhancing interpersonal functioning.
The selection of the most appropriate therapeutic approach depends on the specific disorder, individual needs, and clinical presentation.
Drive Theory and Addiction
Drive theory offers a compelling framework for understanding addiction, suggesting that addictive behaviors are driven by powerful, often overwhelming, biological and psychological needs. These needs, once activated, create a state of tension or arousal that compels individuals to engage in substance use or other addictive behaviors to achieve relief or gratification. This process, while seemingly simple, involves complex interactions between neurobiological systems and learned behaviors.Addictive behaviors can be effectively analyzed through a drive-reduction lens.
The initial use of a substance or engagement in an addictive behavior might be driven by a variety of factors, ranging from social pressure to curiosity. However, repeated engagement leads to the development of strong associations between the behavior and the reduction of negative emotional states (such as stress, anxiety, or depression) or the enhancement of positive ones (such as euphoria or pleasure).
This creates a powerful negative feedback loop; the unpleasantness of craving intensifies the drive to engage in the addictive behavior, and the behavior temporarily reduces the craving. This cycle perpetuates the addiction, with the initial drive becoming increasingly intertwined with the biological and psychological mechanisms of reward and reinforcement.
Neurobiological Mechanisms in Addictive Drives
The neurobiological underpinnings of addictive drives are centered around the brain’s reward system, particularly the mesolimbic pathway. This pathway, involving the ventral tegmental area (VTA), nucleus accumbens, and prefrontal cortex, is crucial in processing pleasure, motivation, and reward. Addictive substances and behaviors hijack this system, leading to the release of dopamine, a neurotransmitter associated with feelings of pleasure and reinforcement.
Repeated exposure to the addictive substance or behavior sensitizes the reward system, requiring progressively higher levels of stimulation to achieve the same level of reward. This sensitization contributes to the escalating nature of addiction, leading to tolerance and dependence. Furthermore, the brain’s stress response system is also heavily implicated, with the release of cortisol and other stress hormones reinforcing the association between the addictive behavior and stress reduction.
For example, individuals experiencing high levels of anxiety might turn to alcohol or drugs to alleviate these feelings; the initial relief reinforces the behavior, creating a powerful cycle of stress and substance use. The prefrontal cortex, responsible for executive functions such as decision-making and impulse control, is also significantly affected, weakening the ability to resist the urge to engage in addictive behaviors, even when the individual recognizes the negative consequences.
Criticisms of Drive Theory
Drive theory, while influential in understanding motivation, has faced significant criticisms over the years. Its core tenets, emphasizing biological needs and drive reduction, have been challenged by alternative perspectives that consider cognitive and social factors. This section will explore these limitations and contrast drive theory with other motivational frameworks.
Limitations and Weaknesses of Drive Theory
Drive theory’s power is limited by several key weaknesses. These limitations impact its ability to accurately predict and explain human behavior in diverse contexts.
- Oversimplification of Motivation: Drive theory simplifies the complexity of human motivation by focusing primarily on biological needs. It often overlooks the influence of cognitive factors such as goals, expectations, and beliefs, which significantly shape our actions. For example, a student might study hard not solely to reduce the drive of hunger (a biological need), but also to achieve the goal of getting good grades and securing a scholarship (cognitive factors).
- Inflexibility in Explaining Non-Biological Drives: Drive theory struggles to account for motivations not directly tied to biological needs, such as the drive for achievement, affiliation, or power. The intense desire to climb Mount Everest, for instance, isn’t easily explained by a simple drive reduction model. The motivation is rooted in personal goals and aspirations rather than a biological imperative.
- Neglect of Environmental Influences: The theory largely ignores the role of environmental factors in shaping motivation. Learned behaviors and cultural norms often influence our choices, overriding basic biological drives. For example, despite a strong biological drive for hunger, an individual might choose to skip a meal due to societal expectations surrounding fasting during religious observances.
- Difficulty in Explaining Behaviors without an Apparent Drive: Drive theory has trouble explaining behaviors that don’t seem to serve any immediate biological need, such as curiosity or exploration. A child’s innate curiosity to explore their surroundings, for instance, cannot be fully explained by the drive reduction model; the behavior isn’t directly reducing a biological drive.
- Lack of Consideration for Individual Differences: The theory doesn’t adequately account for individual differences in motivation. People vary in their thresholds for different drives and their responses to stimuli. For instance, two individuals might experience the same level of thirst, yet one might feel a stronger drive to drink water than the other due to factors like personality or past experiences.
These limitations significantly reduce the predictive power of drive theory. While it can explain some basic behaviors driven by biological needs, it fails to capture the richness and complexity of human motivation in most real-world situations.
Alternative Theories of Motivation
Several alternative theories offer more comprehensive explanations of motivation by incorporating cognitive and social factors that drive theory largely ignores.
| Theory Name | Core Principles | Strengths | Weaknesses | Key Differences from Drive Theory |
|---|---|---|---|---|
| Expectancy Theory | Motivation is determined by the expectancy of success, instrumentality (belief that success leads to rewards), and valence (value of the reward). | Accounts for cognitive factors; explains effort in goal-directed behavior. | Can be complex to apply; assumes rationality in decision-making. | Focuses on cognitive appraisals rather than biological drives; emphasizes conscious choices. |
| Self-Determination Theory | Motivation is influenced by intrinsic and extrinsic factors, with intrinsic motivation being more self-determined and sustainable. | Highlights the importance of autonomy, competence, and relatedness; explains the persistence of behavior. | Can be difficult to measure intrinsic motivation; doesn’t fully address the role of biological needs. | Emphasizes the importance of psychological needs and autonomy, rather than solely biological drives. |
| Goal-Setting Theory | Specific, challenging, and attainable goals enhance performance and motivation. | Provides a practical framework for improving motivation; emphasizes the role of conscious goals. | Doesn’t fully account for emotional factors; assumes individuals have the resources to achieve their goals. | Focuses on conscious goal-setting and achievement, unlike the automatic drive reduction process. |
For example, expectancy theory better explains a salesperson’s motivation to make sales than drive theory. The salesperson is driven by the expectation of earning a commission (reward) for meeting sales targets (expectancy), rather than solely by the reduction of a biological drive. Self-determination theory would highlight the importance of providing autonomy to the salesperson to enhance their intrinsic motivation.
Goal-setting theory would focus on setting clear, challenging, and attainable sales targets. These alternative theories address the limitations of drive theory by considering cognitive factors, individual differences, and the impact of the environment.
Drive Theory Compared with Other Motivational Frameworks
Drive theory can be contrasted with other frameworks, such as Maslow’s Hierarchy of Needs and Herzberg’s Two-Factor Theory. Maslow’s hierarchy posits a hierarchical arrangement of needs, starting from basic physiological needs to self-actualization. Herzberg’s theory differentiates between hygiene factors (preventing dissatisfaction) and motivators (promoting satisfaction). Drive theory primarily focuses on the physiological level of Maslow’s hierarchy and overlaps with the hygiene factors of Herzberg’s theory.
However, it lacks the scope of Maslow’s broader perspective on human needs and ignores the motivators identified by Herzberg. A Venn diagram could illustrate the overlap between drive theory and Maslow’s hierarchy, showing a substantial overlap in the physiological needs area but a significant divergence in the higher-order needs. Drive theory is most applicable when explaining behaviors directly related to biological needs, while Maslow’s hierarchy provides a more holistic view of human motivation, and Herzberg’s theory is useful in understanding job satisfaction and motivation in the workplace.
Drive Theory and Modern Applications
Drive theory, while a foundational concept in psychology, continues to inform contemporary research and applications across various fields. Its emphasis on internal states motivating behavior remains relevant, particularly when considering the interplay between biological needs and learned responses. Modern interpretations often integrate drive theory with other perspectives, such as cognitive and social learning theories, leading to a more nuanced understanding of motivation.While the original formulations of drive theory might seem simplistic in light of contemporary knowledge, its core principles—the interplay between biological needs, homeostasis, and learned behaviors—provide a valuable framework for understanding a range of human behaviors.
Current research builds upon these foundations, refining and expanding our understanding of the complexities of motivation.
Applications in Health Psychology
Drive theory’s principles are readily apparent in health psychology, particularly in understanding health behaviors like adherence to medical regimens or engaging in healthy lifestyles. For example, the drive to reduce discomfort (e.g., pain associated with an illness) motivates individuals to seek medical treatment and follow prescribed medications. Conversely, the drive for pleasure (e.g., the enjoyment derived from smoking or consuming unhealthy foods) can counteract health-promoting behaviors.
Interventions often focus on modifying these drives, either by reducing the negative consequences associated with unhealthy behaviors or enhancing the rewards associated with healthy ones. Research exploring the effectiveness of incentive-based programs to encourage healthy habits, such as weight loss programs that reward progress, directly applies drive theory principles.
Applications in Consumer Behavior
Understanding consumer behavior often relies on principles derived from drive theory. Marketing strategies frequently leverage the concept of drive reduction, appealing to consumers’ needs and desires to motivate purchasing decisions. Advertisements often highlight the satisfaction or pleasure associated with a product, directly targeting the drive for pleasure. For instance, advertisements showcasing the relief from thirst after drinking a beverage or the feeling of comfort from wearing a particular garment directly appeal to the drive-reduction model.
The effectiveness of these strategies underscores the enduring relevance of drive theory in understanding human motivations in a consumer context. Research in neuromarketing increasingly employs neuroimaging techniques to study brain activity associated with these drives, offering a deeper understanding of the neural mechanisms underlying consumer choices.
Applications in Addiction Research
Drive theory offers a useful framework for understanding addiction. The powerful drives associated with substance use, often overriding other needs and desires, are central to addiction research. The initial use of a substance might be driven by curiosity or social pressure, but continued use often stems from the drive to reduce negative affect (withdrawal symptoms) or enhance positive affect (euphoria).
Relapse prevention strategies often focus on managing these powerful drives, using techniques like cognitive behavioral therapy to help individuals develop coping mechanisms and alternative reward systems. The persistent nature of these drives, even in the face of negative consequences, underscores the importance of understanding the biological and psychological mechanisms underlying them. Studies exploring the neurobiological mechanisms of reward and reinforcement in addiction directly utilize and refine the principles of drive theory.
Drive Theory and Hunger

Hunger, a fundamental human drive, exemplifies the interplay between biological and psychological factors within the framework of drive theory. Understanding the mechanisms behind hunger provides valuable insight into the broader principles of drive reduction and homeostasis. This section explores the physiological and psychological processes that contribute to the experience of hunger and its regulation.Biological and Psychological Factors Contributing to HungerHunger is not simply a matter of an empty stomach.
A complex interplay of biological signals, environmental cues, and learned behaviors contributes to our sensation of hunger and our subsequent eating patterns. Biological factors include hormonal fluctuations and neural pathways within the brain, while psychological factors encompass learned associations with food, emotional states, and social influences. The body’s intricate regulatory system constantly monitors energy levels and adjusts accordingly, ensuring sufficient energy for bodily functions.
However, learned behaviors and environmental factors often override these biological signals, leading to imbalances in energy intake and expenditure.
Hormonal Regulation of Hunger
Several hormones play crucial roles in regulating hunger and satiety. Ghrelin, secreted by the stomach, stimulates appetite, increasing hunger levels. Leptin, produced by fat cells, signals satiety, reducing hunger. Insulin, released by the pancreas, helps regulate blood glucose levels, influencing both hunger and energy storage. These hormones act in concert, creating a feedback loop that maintains energy balance.
Dysregulation of these hormones can lead to imbalances in appetite and contribute to conditions like obesity. For instance, individuals with leptin resistance may experience persistent hunger despite having adequate body fat.
Brain Regions Involved in Hunger Regulation
The hypothalamus, a region in the brain, acts as a central control center for hunger regulation. Specifically, the lateral hypothalamus (LH) stimulates hunger, while the ventromedial hypothalamus (VMH) signals satiety. These areas receive input from various sources, including hormonal signals and sensory information about food. Other brain regions, such as the amygdala and prefrontal cortex, also play roles in influencing food choices and eating behavior, processing emotional aspects and higher-order decision-making, respectively.
Damage to specific areas of the hypothalamus can significantly disrupt eating patterns, leading to either hyperphagia (excessive eating) or aphagia (loss of appetite).
Feedback Loop in Hunger Regulation
The following flowchart illustrates the feedback loop involved in hunger regulation:[Flowchart Description: The flowchart begins with a “Low Blood Glucose” box, which triggers the release of Ghrelin from the stomach. This increase in Ghrelin signals the Lateral Hypothalamus (LH) in the brain, leading to increased hunger. The individual then eats, resulting in an increase in blood glucose.
This increase stimulates the release of Insulin from the pancreas and Leptin from fat cells. Insulin helps regulate blood glucose levels, while Leptin signals the Ventromedial Hypothalamus (VMH) in the brain, leading to decreased hunger and satiety. The loop then returns to the “Low Blood Glucose” box if energy stores are depleted.]
Drive Theory and Thirst
Drive theory posits that physiological needs create internal states of tension (drives) that motivate organisms to engage in behaviors that reduce these drives and restore homeostasis. Thirst, a fundamental drive, provides a compelling example of this theory in action, illustrating the complex interplay between physiological mechanisms, neural pathways, and behavioral responses. Understanding the intricacies of thirst regulation offers valuable insights into the broader principles of drive theory and its application to human behavior.
Thirst, the sensation prompting us to drink, is a crucial mechanism for maintaining fluid balance. This process is not simply a matter of detecting low water levels but involves a sophisticated interplay of physiological sensors, hormonal responses, and neural pathways. Two primary types of thirst, osmotic and hypovolemic, are distinguished by their underlying physiological triggers and subsequent responses.
Physiological Mechanisms of Thirst
The body employs several mechanisms to detect and respond to fluid imbalances, initiating thirst when necessary. These mechanisms can be broadly categorized as osmotic, hypovolemic, and cellular responses.
Osmotic Thirst
Osmoreceptors, specialized neurons located in the organum vasculosum of the lamina terminalis (OVLT) and subfornical organ (SFO), detect changes in extracellular fluid osmolarity. An increase in solute concentration (e.g., due to dehydration or excessive salt intake) causes water to move out of these osmoreceptors, shrinking them and triggering neural signals. These signals are transmitted to the hypothalamus, specifically the preoptic area, activating thirst and promoting vasopressin (antidiuretic hormone) release from the posterior pituitary.
Vasopressin acts on the kidneys to increase water reabsorption, reducing urine output and helping to restore fluid balance. Angiotensin II, a hormone produced in response to low blood volume, also contributes to osmotic thirst, acting synergistically with osmoreceptors to stimulate thirst centers in the brain. A simplified diagram would show osmoreceptors in the OVLT/SFO detecting increased solute concentration, sending signals to the hypothalamus, leading to vasopressin release from the posterior pituitary, resulting in increased water reabsorption in the kidneys.
Hypovolemic Thirst
Hypovolemic thirst arises from a decrease in blood volume and pressure. Baroreceptors, located in the carotid sinus and aortic arch, detect this decrease and send signals to the brain. Simultaneously, the renin-angiotensin-aldosterone system (RAAS) is activated. Reduced blood flow to the kidneys triggers the release of renin, which initiates a cascade of events leading to the production of angiotensin II.
Angiotensin II acts on both the brain (stimulating thirst) and the adrenal glands (stimulating aldosterone release), which promotes sodium and water retention by the kidneys. A flowchart illustrating RAAS would show reduced blood volume leading to renin release, angiotensin I conversion to angiotensin II, aldosterone release, sodium and water retention, and ultimately increased blood volume. Atrial natriuretic peptide (ANP), released from the heart in response to increased blood volume, counteracts the effects of angiotensin II, promoting sodium and water excretion.
Cellular Mechanisms
Changes in cell volume also play a role in thirst regulation. When extracellular fluid osmolarity increases, water moves out of cells, causing them to shrink and activating specific ion channels and transporters that signal thirst. Aquaporins, water channels in cell membranes, facilitate water movement across cell membranes, influencing the rate at which cells rehydrate and impacting the overall thirst sensation.
Types of Thirst
Osmotic and hypovolemic thirst, while distinct, can sometimes occur simultaneously.
Osmotic Thirst Examples
Osmotic thirst results from situations causing increased extracellular solute concentration, such as dehydration from insufficient water intake or excessive salt ingestion. The physiological response to water deprivation primarily involves increased vasopressin release and decreased urine output. In contrast, hypertonic saline infusion directly increases plasma osmolarity, triggering a rapid and intense thirst response.
Hypovolemic Thirst Examples
Hypovolemic thirst arises from situations causing decreased blood volume, such as hemorrhage (significant blood loss) or severe diarrhea. Hemorrhage triggers a dramatic activation of RAAS and a pronounced thirst response. Sweating, while also causing fluid loss, results in a less intense thirst response compared to hemorrhage because it primarily involves water loss with less significant changes in blood volume.
Simultaneous osmotic and hypovolemic thirst can occur during prolonged dehydration or severe blood loss, where both extracellular solute concentration and blood volume are reduced.
Neural Pathways in Thirst Sensation
The brain integrates information from various sources to regulate thirst.
Brain Regions Involved
The hypothalamus, particularly the preoptic area, supraoptic nucleus, and paraventricular nucleus, plays a central role in thirst regulation. Circumventricular organs like the OVLT and SFO, which lack a blood-brain barrier, are crucial for detecting changes in blood osmolarity. The amygdala also contributes by associating thirst with emotional states. A diagram would illustrate these regions and their interconnections, showing the flow of information from peripheral sensors to the hypothalamus and other brain regions.
Neural Circuits
Peripheral sensors (osmoreceptors, baroreceptors) send signals via neural pathways to the brain, utilizing neurotransmitters such as glutamate and GABA. The brain integrates information from multiple pathways, modulating thirst based on factors like fluid balance, energy expenditure, and other physiological needs. Higher brain centers, such as the cortex, exert top-down control over thirst behavior, influencing conscious decisions about fluid intake.
Comparative Table
| Feature | Osmotic Thirst | Hypovolemic Thirst |
|---|---|---|
| Stimulus | Increased extracellular solute concentration | Decreased blood volume and pressure |
| Receptors | Osmoreceptors | Baroreceptors, renin-angiotensin system |
| Hormonal Response | Vasopressin release | Renin-angiotensin-aldosterone system activation |
| Primary Effect | Cellular dehydration | Reduced blood pressure and volume |
Further Considerations
Impaired thirst mechanisms can have severe consequences. Diabetes insipidus, for instance, involves insufficient vasopressin production, leading to excessive water loss and intense thirst. Hypodipsia, characterized by reduced thirst sensation, can be life-threatening if left untreated. Aging can also affect thirst regulation, potentially increasing the risk of dehydration in older adults. The ethical implications of manipulating thirst pathways for therapeutic purposes require careful consideration, balancing potential benefits with potential risks and ensuring patient autonomy.
Essential Questionnaire
What are some common criticisms of drive theory?
Drive theory has been criticized for its oversimplification of human motivation, neglecting cognitive and social factors. It struggles to explain behaviors not directly tied to biological needs and fails to fully account for the influence of learned behaviors and environmental factors on motivation.
How does drive theory relate to addiction?
Addiction can be viewed through a drive-reduction framework, where the drug use temporarily reduces the intense craving (drive) for the substance. However, the repeated reinforcement of this behavior and the neurobiological changes associated with addiction make it a complex phenomenon that goes beyond simple drive reduction.
Does drive theory account for individual differences in motivation?
While the basic tenets of drive theory apply across individuals, it’s acknowledged that individual differences in genetics, personality, and experiences significantly modulate the strength and expression of drives. These differences affect how individuals respond to drive states and the behaviors they employ to reduce those states.
How does drive theory differ from incentive theory?
Drive theory emphasizes internal states pushing an organism towards behavior, while incentive theory focuses on external stimuli pulling the organism towards a reward. Both theories contribute to a complete understanding of motivation, with drive theory explaining the push from internal needs and incentive theory explaining the pull from external rewards.

